[Up to Main]
Some people think that a mental disorder of some sort might be at the root of their asexuality. After all, something like Hypoactive Sexual Desire Disorder sounds very much like asexuality when you read about it.
Before we dive into that, let me first say that even in the case where there is something that makes you feel asexual, that doesn’t prohibit you from using the word. If this is who you are, if this word accurately describes you and you find value in using the word, then you are allowed to use it, regardless of whether or not there’s some underlying reason.
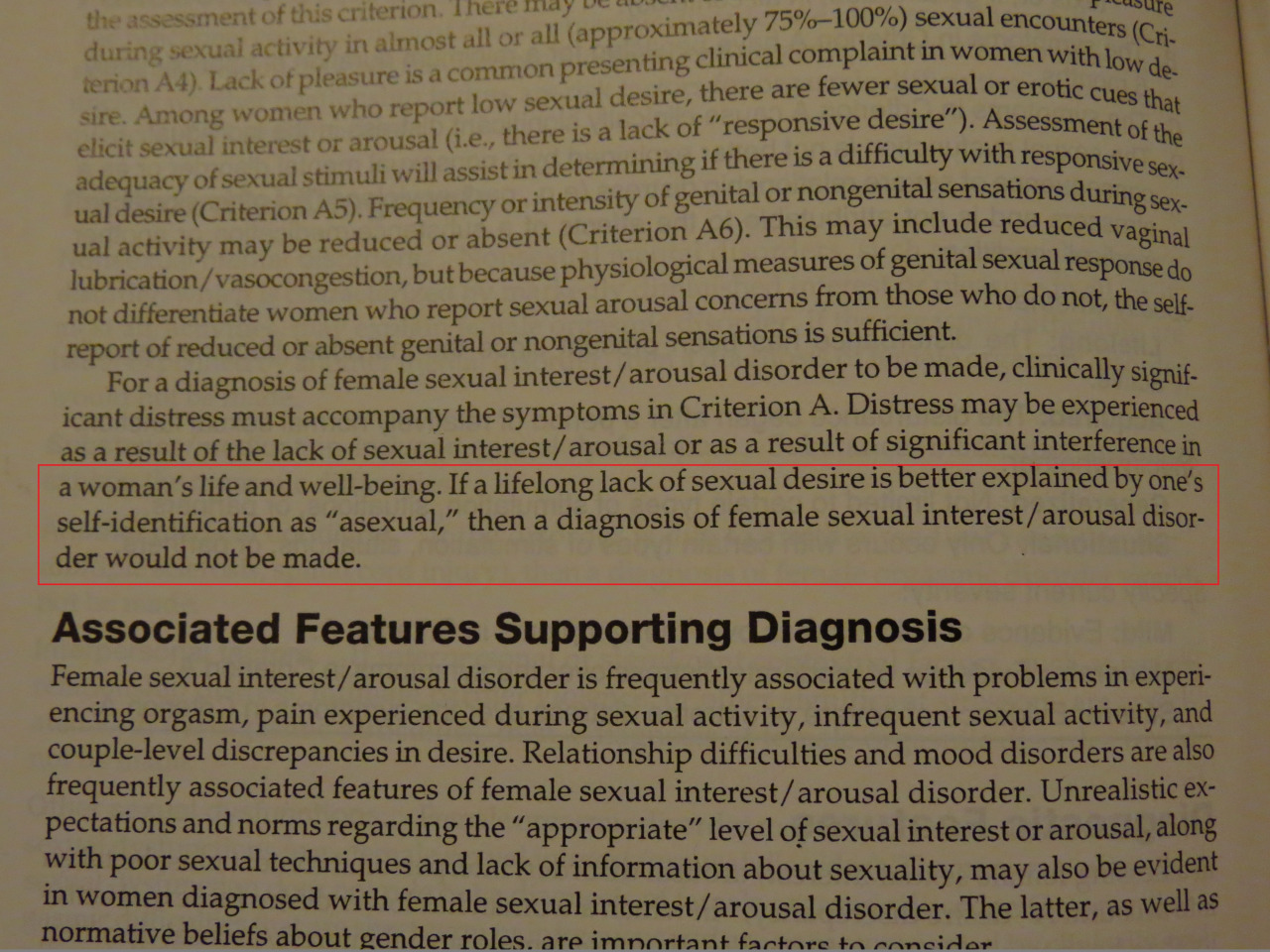
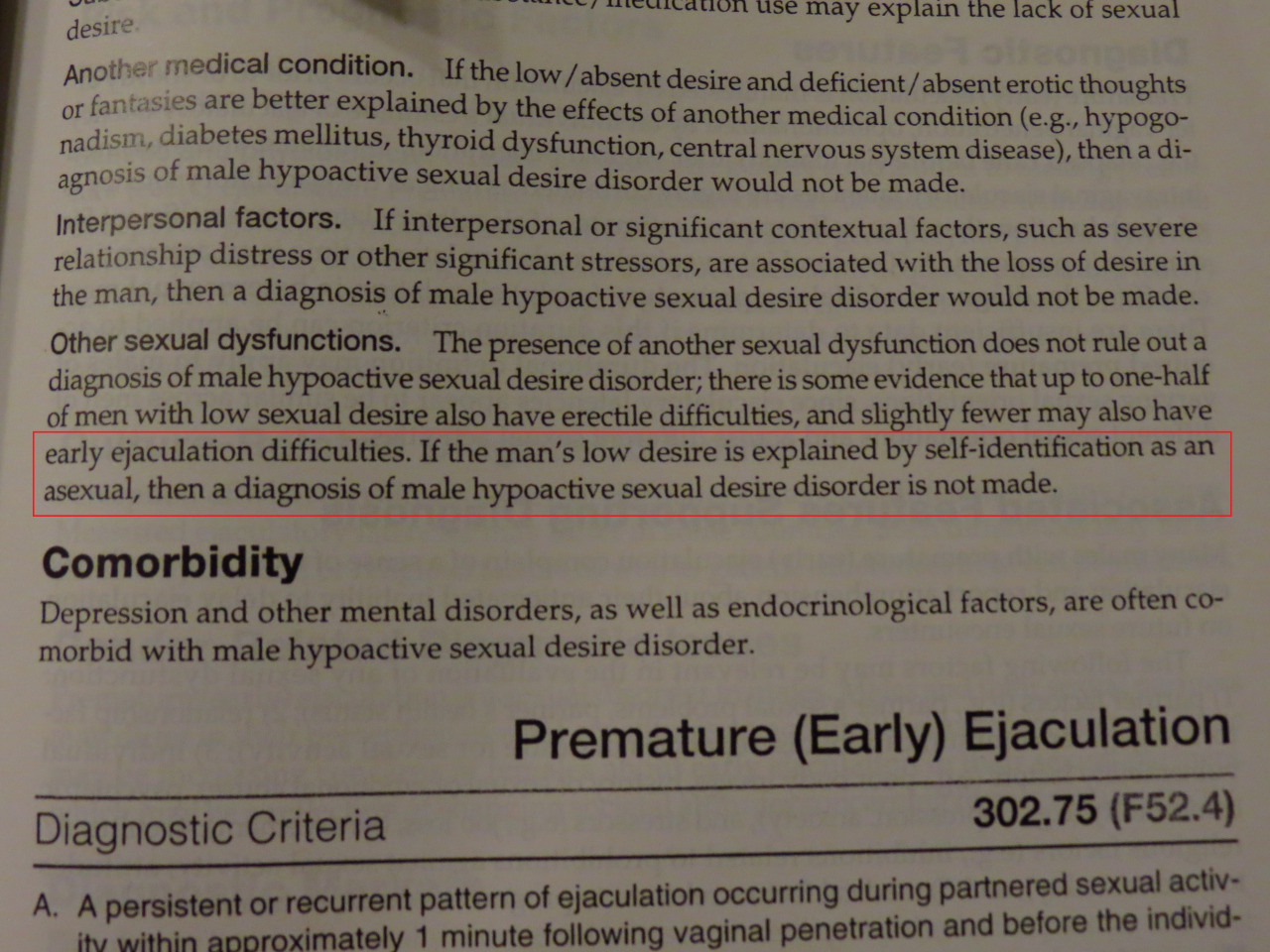
Now, it is true that there are a number of conditions described in the DSM have criteria which sound like they’re talking about asexual people. Hypoactive Sexual Desire Disorder lists “persistently deficient sexual/erotic thoughts or fantasies and desire for sexual activity”. Female Sexual Interest/Arousal Disorder lists “Absent/reduced interest in sexual activity. Absent/reduced sexual/erotic thoughts or fantasies.” (FSA/ID is actually the combination of two diagnoses listed separately in an earlier edition of the DSM. For some reason, they combined a lack of sexual interest, which is a mental thing, and a lack of sexual arousal, which is a physical thing. That seems like an odd pair of things to combine.) Schizoid Personality Disorder lists “Has little, if any, interest in having sexual experiences with another person.” And those aren’t the only conditions with similar descriptions, and the DSM isn’t the only diagnostic guide, these are just a sample of what’s out there.
So, there are things that psychiatric manuals describe in words that make them sound similar to asexuality. What does that mean?
Maybe not as much as you think. There are two important things to keep in mind.
- All of these guides and diagnostic manuals are descriptions based on observations. They are based on the idea of a mythical “normal” person, and any deviation from that is noted. If they start seeing a pattern of these deviations, it can get labeled a “disorder”. This is called “pathologization”.
- These guides are not infallible. There have been five major revisions of the DSM so far. Some “disorders” are dropped, some are added, and some are refined to take into account new discoveries or new understandings. There are things that are in the DSM-5 today that are flat out wrong and which will be removed in the next edition.
With that in mind, let’s look at how asexuality fits into this model.
First, between DSM-IV and DSM-5, the HSDD and FSI/AD descriptions were drastically changed and restructured. One of the primary additions was and explicit exception that says that someone should not be diagnosed with either one, if they self-identify as asexual. So that’s a direct recognition that asexuality is not HSDD or FSI/AD. And one of the main things that was removed was the part of the diagnostic criteria that considered a partner’s distress. Under the DSM-IV, someone could be diagnosed if their partner were distressed by the person’s lack of sexual interest, even if the person themselves were perfectly fine with it. So, the DSM-5 has fixed some of the more egregious problems in the DSM-IV and that’s good, but that’s not enough. Someone still has to know about asexuality in order to be able to “self-identify” as asexual. If they’re ace, but have never heard the word before, they’ll get marked as having “Lifelong Generalized” HSDD or FSI/AD. Why should a diagnosis depend on your vocabulary?
Let’s take a step back. In point #1, I noted that things get into these guides because people notice patterns and put a name and some diagnostic criteria to them, and call them a “disorder”. But in the case of HSDD and the “Interest” part of FSI/AD, maybe the pattern they’re describing actually is asexuality, and the only reason it’s listed at all is that no one really had the words to talk about it, so no one really understood it. It became pathologized and called a disorder, instead of being recognized as a perfectly normal thing that a lot of people are. And now that we have the words, we’re able to talk about it, we’re able to find others who feel the same way, and we’re able to say, “Hey, that sounds an awful lot like us, and there’s nothing wrong with us, so stop saying we have a problem.”
“What about distress?”, you say? What if someone is distressed about their “Absent/reduced interest in sexual activity” or whatever? Look at the source of that distress. Very often, the source is the pathologization itself. You are repeatedly told that everyone wants sex and everyone likes sex and that everyone will have sex and that everyone will find someone that they want sex with. You are expected to provide a partner with an adequate and regular supply of mutually desirable sex. TV, books, movies, music, friends, coworkers, all of it drills this message into your head. So, if you realize that you don’t fit these expectations, that none of that is really part of your world, and you don’t know why and no one tells you that it’s okay, then of course you’re going to feel distressed. Even when someone tells you that it’s okay, because the rest of the world still tells you that it’s not.
[Up to Main]